Shoulder Arthritis (Shoulder Osteoarthritis)
Shoulder osteoarthritis (OA) is a degenerative joint disease that affects the cartilage and bones in the shoulder joint. Over time, the protective cartilage that covers the ends of the bones in the shoulder wears down, leading to pain, stiffness, and reduced mobility. Osteoarthritis of the shoulder is less common than OA in weight-bearing joints like the knee or hip but can still significantly impact quality of life and affect patients that engage in repetitive overhead shoulder motions.
The shoulder is a complex and highly mobile joint that allows for a wide range of motion. It consists of three bones: the clavicle (collarbone), scapula (shoulder blade), and humerus (upper arm bone). These bones form the following key joints:
- Glenohumeral Joint: This is the ball-and-socket joint where the head of the humerus (ball) fits into the glenoid cavity of the scapula (socket). It is the primary joint affected by osteoarthritis in the shoulder.
- Acromioclavicular Joint: Where the clavicle meets the acromion (part of the scapula). This joint may also be involved in shoulder OA.
- Sternoclavicular Joint: Where the clavicle connects to the sternum (breastbone), although it is less commonly affected in OA.
The joint is stabilized by ligaments, muscles, and tendons, including the rotator cuff muscles, which are crucial for shoulder function. The rotator cuff consists of four muscles—supraspinatus, infraspinatus, teres minor, and subscapularis—that help maintain the stability of the shoulder during movement.
Osteoarthritis occurs when the cartilage that cushions the ends of bones gradually wears away. In the case of shoulder osteoarthritis, this degeneration most commonly affects the glenohumeral joint. The cartilage that normally allows smooth motion of the shoulder joint breaks down, and bone surfaces begin to rub against each other. This can lead to the formation of bone spurs, inflammation, and pain.
Osteoarthritis can develop for several reasons, including:
- Age
- Previous Shoulder Injury: A history of shoulder trauma, such as fractures or dislocations, increases the risk of developing OA.
- Repetitive Use: Occupations or activities that involve repetitive overhead motions (e.g., athletes, manual laborers) may contribute to joint wear and tear.
- Genetics: Family history of OA can predispose individuals to developing the condition.
- Inflammatory Conditions: Conditions like rheumatoid arthritis can increase the likelihood of developing shoulder OA.
The symptoms of shoulder osteoarthritis can vary in severity depending on the degree of cartilage damage and the overall condition of the joint. Common symptoms include:
- Pain: Pain is typically the most prominent symptom. It can occur gradually and worsen over time. The pain may be felt in the front or deep within the shoulder, and can radiate down the arm or into the upper back. It is often aggravated by activities that require arm movement, especially overhead or heavy lifting.
- Stiffness: A reduction in the range of motion is common. Individuals with shoulder OA often experience difficulty raising their arm, reaching behind their back, or performing tasks that require arm movement.
- Swelling: Inflammation of the joint can lead to noticeable swelling around the shoulder, making the joint feel tender or warm to the touch.
- Grinding or Cracking Sounds: As the cartilage deteriorates, bone surfaces can rub together, leading to a grinding sensation or popping sounds (crepitus) when moving the arm.
- Weakness: Weakness in the shoulder muscles, particularly the rotator cuff, can develop due to pain, disuse, or the breakdown of joint structures.
Management of shoulder osteoarthritis typically begins with nonsurgical treatments aimed at reducing pain and improving function. Some effective nonsurgical options include:
- Physical Therapy: A physical therapist can guide patients through exercises to improve flexibility, strengthen the muscles surrounding the shoulder, and restore range of motion. Stretching and strengthening the rotator cuff and scapular muscles are essential components of therapy.
- Medications: Over-the-counter medications like acetaminophen (Tylenol) or nonsteroidal anti-inflammatory drugs (NSAIDs) such as ibuprofen (Advil, Motrin) can help manage pain and inflammation. In more severe cases, doctors may prescribe stronger pain relievers or corticosteroid injections.
- Corticosteroid Injections: In some cases, a corticosteroid injection into the shoulder joint may help reduce inflammation and provide temporary pain relief. This can improve function and provide a period of symptom relief, but repeated injections should be limited due to potential side effects.
- Joint Supplements: Supplements like glucosamine and chondroitin sulfate are commonly used, although evidence supporting their effectiveness is mixed. They may provide some relief by promoting cartilage health and reducing inflammation.
- Heat or Cold Therapy: Applying heat or cold to the shoulder can help manage pain and swelling. Cold packs are typically used for acute pain or swelling, while heat packs are more helpful for chronic stiffness.
When nonsurgical treatments fail to provide adequate relief and quality of life is significantly impacted, surgical intervention may be necessary. Surgical options for shoulder OA include:
- Arthroscopic Debridement: Used in rare cases but in this minimally invasive procedure, small incisions and a camera are used to view and remove damaged tissue, bone spurs, or inflamed synovial tissue within the joint. While it may provide relief for some patients, it is typically only beneficial in the early stages of OA.
- Shoulder Arthroplasty (Total Shoulder Replacement): In cases of advanced OA where the cartilage has completely worn away, a total shoulder replacement may be considered. During this procedure, the damaged parts of the joint are replaced with artificial components made of metal, plastic, or ceramic. This surgery is highly effective in relieving pain and improving function
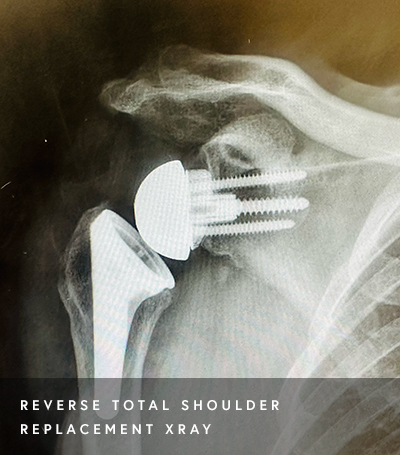
- Reverse Shoulder Arthroplasty: This is an option for individuals with severe OA, particularly those who have a rotator cuff tear in addition to arthritis. In a reverse shoulder replacement, the ball and socket are switched to allow the deltoid muscle to compensate for the rotator cuff deficiency. This procedure is particularly beneficial for people who have significant shoulder dysfunction.
Shoulder osteoarthritis is a condition that can significantly impair an individual’s daily activities, causing pain, stiffness, and limited mobility. Understanding the anatomy of the shoulder, recognizing the symptoms, and exploring treatment options is crucial for managing this condition. Treatment approaches are often dependent on individual patient goals. Nonsurgical approaches, including physical therapy and medications, are often effective in the early stages of OA. For more advanced cases, surgical options like shoulder replacement may be necessary to restore function and relieve pain. Early diagnosis and appropriate treatment can help maintain shoulder health and improve the quality of life for those affected by shoulder osteoarthritis.
At a Glance
Dr. Hasani Swindell
- Fellowship-Trained Sports Medicine Specialist
- Board-Certified Orthopedic Surgeon
- Summa Cum Laude Graduate from the University of Pittsburgh
- Medical Degree from Columbia University
- Learn more