ACL Tear
An anterior cruciate ligament (ACL) tear is a common knee injury that often occurs during sports or high-impact activities. Specifically, it can be seen in activities that involve jumping, pivoting or change of direction movements. The ACL is one of the key ligaments that stabilizes the knee, and when it tears, it can cause pain, instability, and impaired athletic performance. ACL injuries are particularly common in young, active individuals involved in sports like soccer, football, basketball, and skiing.
Treatment options include both nonoperative and surgical approaches, depending on the severity of the tear, the patient’s activity level and desired goals after injury. Surgical reconstruction of the ACL is common and often recommended, especially in active patients. Typically ACL reconstruction offers excellent long-term outcomes and allows return to sports and physical activity.
ACL reconstruction is typically recommended for:
- Young and active individuals who want to return to sports
- Patients with knee instability
- Associated injuries (e.g., meniscus tears, MCL tears)
- High-risk occupations (e.g., firefighting, military, manual labor)
- Failure of nonoperative treatment
ACL tears do not heal on their own. Primary repair can be an option in selected patients however reconstruction has been most predictable in terms of outcomes. Reconstruction involves using a graft to replace the torn ligament.
Surgical Technique:
- Performed arthroscopically (minimally invasive)
- Torn ACL is removed
- Tunnels are drilled in the femur and tibia
- A graft is passed through the tunnels and fixed with screws or buttons
- The new graft acts as a scaffold for new tissue to grow
The choice of graft depends on age, activity level, preference, and surgeon expertise. Common graft types include:
Autograft (from the patient’s own tissue)
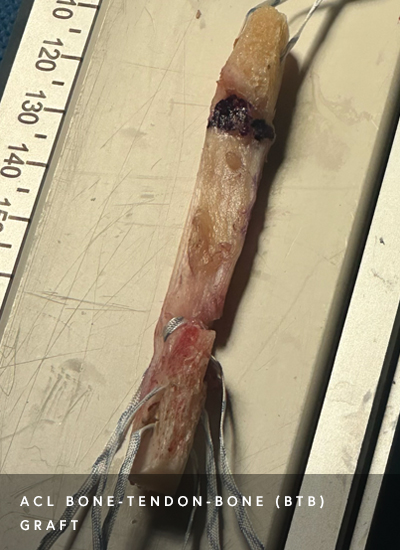
Patellar Tendon Autograft
- Taken from the central third of the patellar tendon
- Strong and reliable graft
- Pros:
- Strong fixation
- Long history of success
- Cons:
- Risk anterior knee pain
- Risk of kneecap fracture (small)
Quadriceps Tendon Autograft
- Gaining popularity for primary and revision surgeries
- Pros:
- Large graft size
- Low donor site pain
- Cons:
- Potential quadriceps weakness
Hamstring Tendon Autograft
- Taken from the semitendinosus and gracilis tendons
- Pros:
- Less pain at the front of the knee
- Smaller incision
- Cons:
- May have slower graft incorporation
- Potential hamstring weakness
- Risk of graft laxity over time
Allograft (donor tissue from a cadaver)
- Used in older or less active patients
- Pros:
- No donor site pain
- Shorter surgery time
- Cons:
- Slightly higher risk of graft failure in young active patients
- Slower incorporation
ACL surgery is an outpatient procedure. Recovery typically follows a structured timeline:
0–2 weeks:
- Use of crutches and knee brace
- Swelling control
- Begin gentle motion exercises
2–6 weeks:
- Gradual increase in motion and strength
- Weaning off crutches and brace
2–6 months:
- Advanced strengthening
- Sport-specific drills
6–12 months:
- Return to running (~4–6 months)
- Return to sports (~9–12 months), guided by functional testing
Rehabilitation is critical for a successful outcome. Adherence to physical therapy is as important as the surgery itself.
- Success rate: Over 85–90% of patients return to pre-injury activity levels
- Athletes can return to competitive sports with proper rehab
- Graft failure rates:
- Lowest in patellar and quadriceps autografts
- Slightly higher in hamstring and allografts, especially in younger athletes
- Risk of re-tear: ~5–10%, higher in younger patients and those returning to pivoting sports
- Long-term outcomes:
- Some patients may still develop arthritis years after injury
- Early reconstruction may protect the meniscus and cartilage from damage
ACL tears are serious injuries that can lead to long-term instability and functional limitations if not managed appropriately. Nonoperative treatment may be an option for older and less active patients, but surgery is often recommended for athletes or those with instability. ACL reconstruction using an autograft or allograft has a high success rate, especially when combined with dedicated physical therapy.
If you suspect you have torn your ACL, consult with an orthopedic specialist to determine the best treatment plan based on your activity level, age, and goals.
At a Glance
Dr. Hasani Swindell
- Fellowship-Trained Sports Medicine Specialist
- Board-Certified Orthopedic Surgeon
- Summa Cum Laude Graduate from the University of Pittsburgh
- Medical Degree from Columbia University
- Learn more